Mike Wilson | 22 October 2024
No type of cancer causes more mortality around the world than lung cancer. While human smoking habits, and limitations of current medicine play a part, we shouldn’t underestimate the importance of late diagnoses. When lung cancer is found during its earliest malignant stages, around two-thirds of patients can expect to live at least five years and many can expect a full recovery. However, if found at advanced stages, five-year survival figures plummet to only one in twenty.[1]
Societies incur significantly higher costs per lung cancer patient than for patients with other forms of the disease. UK estimates imply lung cancer patients cost three times more than a typical bowel cancer patient, and almost nine times as much as a patient with breast cancer. Lung cancer costs the UK economy £2.4bn (US$3.15bn) per year.[2] This significant cost relates not only to lung cancer’s relatively high prevalence, but also to the typical late stage of diagnosis, necessitating treatments with higher costs.
Cancer screening saves thousands of lives a year but is limited by its breadth. Many countries offer services only for cancers of the breast, bowel and cervix, which typically account for barely one quarter of all cancers. However, in recent years lung screening programmes have joined this list in some locations.
In this article we ask what has prompted this change and explore some of the impacts screening might have on diagnoses, patient outcomes and insurance products. We look at whether evidence from early adopters like South Korea might shed light on what countries currently implementing new programmes, like the UK and Australia, can expect.
Why now?
Introduction of a screening programme requires the ready availability of technology, which is affordable enough to roll out widely, and accurate enough to accelerate the diagnosis of a meaningful number of cases. No programme is perfect, and any benefits will be weighed against the harms caused by overdiagnoses, including unnecessary and costly invasive procedures, and anxiety. Even lung scanning itself carries some risk as it exposes patients to radiation.
In recent years, a glut of evidence has shown that lung cancer screening is worthwhile, though this data took a long time to emerge. Proving that the benefits of screening outweigh its downsides is complex. Gold-standard trials typically use lung cancer-specific mortality as a primary endpoint. They involve follow-up periods of five to ten years. This allows enough mortality to occur naturally, so scientists can statistically ‘prove’ that the technology has had a benefit. But even after this time, and in large trials, the results can struggle to achieve statistical significance. Credible numbers of deaths in late-middle aged trial participants take time to emerge.
For example, the NELSON trial, published in 2020 using data from the Netherlands, found that after a 10-year follow-up, high-risk individuals who had been screened were 24% less likely to die from lung cancer that those who had not been screened, though 95% confidence intervals suggested a reduction of anywhere between 6% and 39%, meaning it was not possible to rule out a far smaller (or larger) benefit. Nonetheless, the results, shown below, added valuable evidence in favour of lung screening.[3]

Lung cancer mortality among male participants in NELSON lung screening trial
Similarly, the UK Lung Screening Trial (2021) accrued only 76 deaths in its 7-year follow-up period. 30 of these happened in people who had been screened, leading to a central estimate of a 35% reduction in lung cancer mortality. But again confidence intervals were wide. In this case they overlapped zero (between 59% benefit and 2% worsening) and so were not strictly statistically significant.[1]
However, several other studies emerged within a few years, all suggesting the same thing. Data came from the United States, Italy, Germany, South Korea and more, with consistent results. In isolation, each trial implied a modest benefit but didn’t have enough data to confidently prove it. However, a meta-analysis of nine of these studies suggested more convincing benefits, estimating a 16% reduction in lung-cancer mortality which did reach clear statistical significance, and a 3% reduction in all-cause mortality which was also (just!) significant.[2]
The nature of lung screening
Modern day lung screening employs low dose computed tomography (LDCT) whose potential was first widely recognised in the 1990s. The scan takes the form of a series of x-rays which, when combined, form a detailed picture of a person’s lungs. The small dosage of radiation allows more frequent scanning with minimal risk. However, because the procedure is not risk free, and uses expensive and scarce medical resources, testing is limited to those at high risk. Australian authorities estimate that patients eligible for LDCT scanning have a 6-year cancer risk of at least 1.5%.
Definitions of high risk differ slightly across territories, but typically involve:
- Age risk: Health services invite people in higher-risk age bands. In the United States this is 50 to 80. In the UK and South Korea this is 55 to 74, and in Australia 50 to 70. The typical age profile of lung cancer is shown below, demonstrating that these are ages with high incidence.
- Behavioural risk: 80-90% of people who get lung cancer are smokers or ex-smokers. To be eligible for LDCT, an individual must have accrued significant smoking history. For example in the United States, they must have smoked within the last 15 years and accumulated at least a 20 ‘pack year history’, meaning the equivalent of 20 cigarettes per day (a pack) for 20 years. In other words they need to have smoked at least 146,000 cigarettes in their life. This threshold can vary. For example the forthcoming Australian programme will only screen those with at least a 30 pack-year history, and at least some smoking within 10 years.
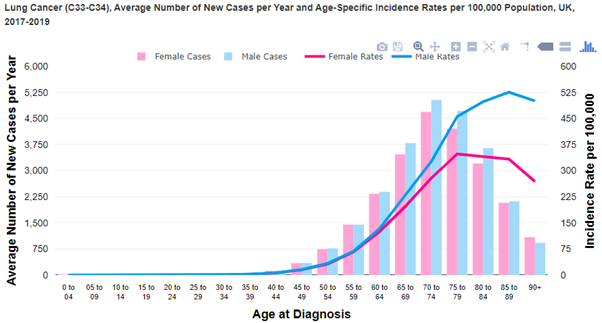
Lung cancer diagnoses are most common in people aged 70 to 79
Current status
Some lung screening programmes are underway. The US Preventive Services taskforce recommended lung screening for some high-risk individuals as long ago as 2015 and widened this recommendation in 2021. A South Korean programme began in 2019 and screening is also well-established in Singapore, and other territories.
In contrast, programmes in many other countries are only beginning now, with a UK programme recently beginning, aiming to reach 40% of the eligible population by 2025, and 100% by 2030.[6] An Australian programme will begin in July 2025[7], and similar programmes are being rolled out around continental Europe.
Although the effectiveness of each programme will depend on entry criteria, uptake levels, and background rates of lung cancer, countries newly adopting this procedure can look to the first movers for guidance on what to expect. Encouragingly, a South Korean study found a material short-term reduction in mortality among those who had lung cancer discovered via screening, and those whose disease was identified via other means.[8] American data is less conclusive, not least because in 2022, it is estimated only 4.5% of those eligible were screened, though this may not fully reflect uptake in the US’ fragmented health system. Despite low uptake, lung screening is estimated to have saved a cumulative 80,000 additional years of life by 2023.[9]
Given the wide-ranging trial evidence, and early real-life evidence in favour of lung screenings, territories adopting these programmes can expect to see modest but significant impacts on mortality. Australian authorities estimate that their programme will prevent over 12,000 lung cancer deaths, and lead to between 30,000 and 50,000 additional quality adjusted life years in its first ten years.[10] When fully active, the UK scheme expects to conduct one million scans and accelerate the diagnoses of 9,000 lung cancers each year.
Other anticipated impacts
The primary aim of these screening services is to lower mortality in the general population. We have seen that they appear likely to successfully achieve this to some extent. However, we can expect other impacts as well, some of which may also be material for insurers.
The challenge of indeterminate findings: Not all LDCT scan results are either ‘cancer’ or ‘all clear’ and the grey areas between these two can present challenges for clinicians, patients and insurers. Supporting information from the fledgling Australian scheme, below, shows some of the anticipated patient pathways. These include both non-malignant lung nodules and incidental findings unrelated to lung cancer.
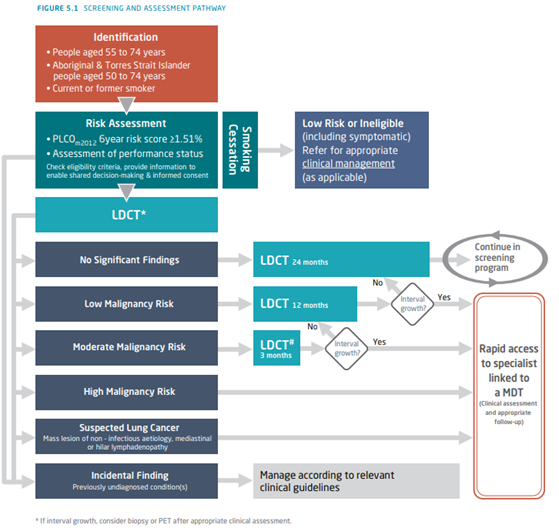
The authors estimate 580,000 Australians (2.2% of the population) will be eligible in each screening cycle and that local health authorities will see positive findings in 11% of scans. This implies 64,000 abnormal findings per screening cycle or – since screenings are every two years – 32,000 per year in the unlikely event everybody participates. Consider that there are only 12,500 cases of lung cancer every year in Australia and you will see that a significant proportion of abnormal findings must be other than confirmed current lung cancer. The same applies in other countries, all of which scan using the same technology.
Pulmonary nodules constitute the majority of anticipated non-cancerous abnormal findings. Around 95% of these nodules are benign. Besides cancer, causes include infections – including scarring from historic infections – pollution and other pulmonary diseases
Due to these findings, many of which would otherwise not have required treatment, estimates suggest overall healthcare costs after introducing LDCT will increase. Despite significant savings associated with diagnoses of cancer at earlier stages, the cost of investigating, and sometimes treating, ‘over-diagnosed’ conditions more than offsets any financial gains.[12]
Pacific Life Re’s underwriting manual, Ocean, contains updated guidance to support the underwriting of a wide variety of potential scenarios arising from applicants with a history of lung screening, across pages covering Pulmonary (Lung) Nodules, Lung and Bronchus Cancer and COPD. Insurers should familiarise themselves with the risks associated with the likely range of findings from LDCT scans and ensure they have robust but fair underwriting philosophies, restricting access to cover only where it is appropriate to do so.
Accelerating diagnoses: A territory with a fully implemented lung screening programme should see a higher proportion of cancers diagnosed at early stages. At present, prior to any screening programme, almost 50% of lung cancers in the UK are diagnosed at the most advanced Stage (4), with a further 20% at Stage 3. US data is shown below. We can expect these proportions to shift towards earlier stages.
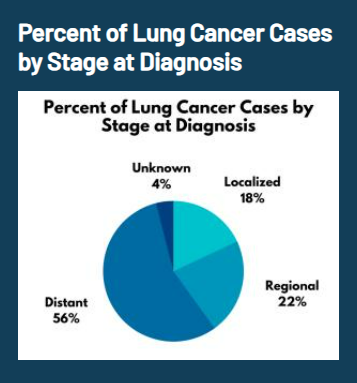
Most lung cancer cases are diagnosed at advanced stages. (US data).
In a population without screening, at any given time there must be many cases of cancers undiagnosed, which would not be found until they become symptomatic or are diagnosed by chance during other investigations. The vast majority of next year’s Stage 4 diagnoses likely already exist now, undetected. During the first sweep through the at-risk population we can therefore expect to see higher numbers of diagnoses as the screening programme does its job and identifies some of these cases.
We see evidence of this in the trials used to prove lung screening works. For example the leading UK study found 86 cancers in the screening arm and fewer - 75 - in its control arm. The Dutch NELSON trial found that after 10 years of follow-up, the incidence of lung cancer was 5.58 cases per 1000 person-years in the screening group and 4.91 cases per 1000 person-years in the control group.
The period of introduction may therefore appear to (artificially) include a higher total number of cases. Insurers offering payments on diagnosis of cancer should be aware of a potential increase, though since this will be a marginal increase for a single site of cancer, we do not anticipate a major impact. Any impact will be less material if take-up is low, and less impactful (i.e. with less of a ‘sudden surge’) if screening programmes are rolled out only slowly.
Diminishing returns: Note that lung screening forms only one item in a pipeline of medical developments which is, after a long period with few advances, looking healthy. Each life can only be saved once, and when quantifying the impact of various developments, we should remember each – including LDCT screening – will exist in a future medical landscape which is different from that in which we live now, and in which key trials to demonstrate their efficacy take place.
For example, any future roll-out of multi-cancer early detection (MCED) blood tests would, to some extent, be fishing from the same pond as LDCT screening. These tests also aim to find cancer at earlier stages, and scientists determine their effectiveness relative to recent historic diagnosis data. If lung screening programmes lead to a shift towards early-stage diagnoses, then this limits the extent to which MCEDs could further improve disease rates, at least for this one cancer site. The same is true for emerging vaccines to prevent lung cancer, the first of which, LungVax, is in early trials.[14]
Smoker differentials: Insurers observe different rates of claim among smokers and non-smokers, which drive differences in pricing in many markets. A successful and popular lung screening programme could materially alter the differential mortality between these two groups. Insurers should ensure they are aware of this possibility and any impacts on pricing of new business or the valuation of existing business.
Conclusion
Lung screening is coming. In several locations, it is already here. The consistency with which territories are now moving to introduce it reflects the fact low dose CT scanning has proved itself as a net social good. In high-risk populations we expect a material shift towards earlier diagnoses, at earlier stages, with related improved survival. This likely outweighs the small but real risks associated with overdiagnosis.
Other impacts naturally flow from this. The process of introducing screening can increase the numbers of diagnoses in the population, especially in the initial years of screening. Health services need to be sure they have the resources to treat these cases, and insurers responding to cancer diagnoses may also see minor impacts. More significantly, lung screening could lead to a far higher number of diagnoses of pre-cancerous or indeterminate tumours.
Of all the cancers, lung cancer has proved one of the toughest nuts to crack. While some innovative treatments show some promise, for many people late diagnosis still exposes them to very poor survival odds. The introduction of safe, effective screening techniques should significantly, if only modestly, shift the odds in favour of less intensive treatment regimes, and longer lives.
[1] Survival for lung cancer | Cancer Research UK
[2] Lung cancer UK price tag eclipses the cost of any other cancer - Cancer Research UK - Cancer News
[6] Lung Cancer Screening | Cancer Research UK
[7] Lung Cancer Screening | Cancer Australia
[9] State of Lung Cancer | Key Findings | American Lung Association
[10] report_on_the_lung_cancer_screening_enquiry_0.pdf (canceraustralia.gov.au)
[11] report_on_the_lung_cancer_screening_enquiry_0.pdf (canceraustralia.gov.au)
[13] Identifying New Biomarkers to Detect Lung Cancer Earlier | Division of Cancer Prevention
[14] New funding for development of world's first lung cancer vaccine | University of Oxford

Mike Wilson
AVP | Medical Analytics






.png)















.png)
.png)




















.png)