Mike Wilson | April 2026

Raised cholesterol is one of the most significant drivers of cardiovascular mortality, along with obesity, raised blood pressure, and high blood sugar. Globally, it causes around 3.6 million deaths each year, which is 6-7% of all deaths.[1] Approximately one quarter of cardiovascular deaths are attributable to high levels of cholesterol. Over time, raised cholesterol can narrow arteries and weaken vessel walls, contributing significantly to heart attacks, as well as strokes, heart failure and other complications.
Treatments today
For decades, the foundation of treatment has been statins. They are cheap, with relatively benign side-effect profiles, widely used, and have already contributed to lower cardiovascular risk in large numbers of people. But they do not eliminate the problem. Some patients continue to have poorly controlled LDL cholesterol despite treatment, while others carry risk from lipid types that statins do little to address.
That is where the next wave of therapies may matter.
What is changing? Emerging treatments for high cholesterol
PCSK9 inhibitors: the most established next step
A significant area of development is PCSK9 inhibitors, a new class of drugs that can reduce LDL cholesterol by around 50–60% – more than double the reduction associated with statins.[2] In the FOURIER trial, evolocumab reduced major cardiovascular events by 20% in high-risk patients already using statins, showing that significant benefit is possible [3].
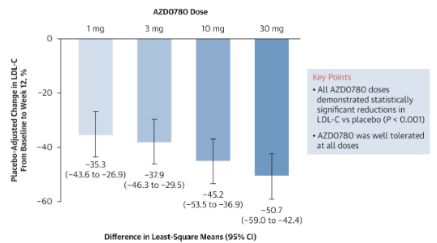
For now, uptake is constrained by cost and the need for injections every two to four weeks. But both barriers may ease over time. As costs come down and patents expire, access could broaden materially. Oral alternatives are also in development, with candidates such as enlicitide decanoate and laroprovstat (formerly AZD0780) showing promising LDL reductions in trials (see below).[4] If successful, these could make the benefits of PCSK9-targeted treatment available to many more patients.
Obicetrapib: promising, but still one to watch
Another notable therapy is obicetrapib, a once-daily pill that lowers LDL through a different mechanism. Obicetrapib targets a natural process which transfers some particles from ‘good’ HDL cholesterol to ‘bad’ LDL. By inhibiting this process, the drug has achieved significant LDL reductions in trials. In the phase 3 BROADWAY trial, it reduced LDL by 30% relative to placebo.[5] When combined with ezetimibe, the reduction approached 50% in the TANDEM trial.[6]
This all sounds promising and the drug’s delivery via a daily pill would be convenient. However, some doubts exist. While obicetrapib appears to improve LDL cholesterol levels, it is less clear whether it reduces the number of LDL particles to the same extent. That may be critical, because particle number is a major driver of cardiovascular risk. In short, the lipid results are promising, but the eventual impact on heart attacks and strokes still needs to be proven.
Lipoprotein(a): the biggest unresolved gap
Around one quarter of people have raised lipoprotein(a), especially those of African, South Asian and Hispanic descent. Unlike standard LDL cholesterol, lipoprotein(a) is largely genetically determined and is not meaningfully improved by diet, exercise or statins. This type of cholesterol contributes to cardiac risks, but there are no available treatments. This could soon change.
Drugs targeting lipoprotein(a) are now in development, including small interfering RNA (siRNA) therapies, to turn off the gene which produces the offending additional protein. Very encouragingly, three different types of treatment all show signs of being effective (see below – the three types are colour coded; one, in blue, has three different candidate drugs).[7]
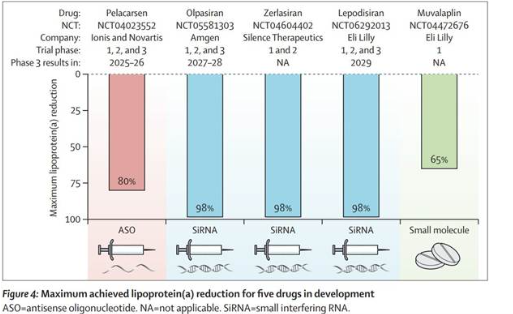
Other candidates involve either short strands of nucleic acids called antisense oligonucleotides (ASOs) which bind to the gene which expresses the unwanted protein; or small molecule therapies which target the protein itself rather than the mechanism through which it is created. The evidence base for these drugs continues to grow. A recent Phase 3 trial showed pelacarsen reduced the need for lipid apheresis, a procedure similar to dialysis, for removing excess lipids from the blood, by over 99%, with 69% of patients requiring no apheresis at all.[8] This drug is the furthest advanced and results from its Lp(a) HORIZON trial are expected this year, with regulatory filings likely to follow soon after.
Why this matters for insurers?
For insurers these drugs could eventually change the impact cholesterol has on mortality and morbidity and contribute to future improvements relating to cardiovascular conditions. Insurers likely reflect these factors in existing improvement assumptions. Effects could be more material when combined with other developments such as weight loss drugs.
For underwriters there may be more subtle changes. If more people can control lipid-related risk successfully, fewer applicants may present with materially raised cholesterol, but those who do could represent a smaller, more treatment-resistant group. A downstream pricing impact associated with these changes would be a modest change to the proportion of lives rated while sharpening the risk profile of the cases that remain.
A further issue is information asymmetry. As awareness and testing of lipoprotein(a) increase, more applicants may know they carry elevated cardiovascular risk even when that is not visible in standard underwriting evidence. American guidelines updated in March 2026 strongly recommend measuring lipoprotein(a) once during an adult’s lifetime. [9]
References
[1] High Cholesterol & Cardiovascular Health | Risks, Prevention, Research & Policy Action
[3] Evolocumab and Clinical Outcomes in Patients with Cardiovascular Disease - PubMed
[4] An Oral PCSK9 Inhibitor for Treatment of Hypercholesterolemia: The PURSUIT Randomized Trial | JACC
[5] Safety and Efficacy of Obicetrapib in Patients at High Cardiovascular Risk - PubMed
[6] Obicetrapib Achieves Robust LDL-C Reductions in Phase 3 ASCVD Trials | HCPLive
[8] Klaus G Parhofer et. Al., Pelacarsen and lipoprotein(a) apheresis in secondary prevention: the Lp(a)FRONTIERS APHERESIS trial, European Heart Journal, 2026;, ehag073,
[9] ACC/AHA Issue Updated Guideline for Managing Lipids, Cholesterol | American Heart Association

Mike Wilson
Director, Medical Analytics






.png)















.png)
.png)




















.png)